|
TRT Seminar Dates: TRT Advanced Workshops: Auriculotherapy Training Dates: |
REWARD DEFICIENCY SYNDROME FACTS AND SOLUTIONS... |
|
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
REWARD DEFICIENCY SYNDROME TOWARD A NEW UNDERSTANDING OF BRAIN FUNCTION: Could Reward Deficiency Syndrome (RDS) be the common psychological thread that links a myriad of compulsive and addictive behaviours? What single trait is shared by… ? addiction to drugs (be they alcohol, cocaine, heroine, marijuana, or cigarettes)
?
? pathological gambling ? sex addiction ? ADHD ? Tourette’s Syndrome ? Autism ? Anorexia and Bulimia ? Being a Workaholic ? Risk-taking behaviours ? and even many of the compulsive disorders? Sound like a trick question? It isn’t. The answer is Reward Deficiency Syndrome (RDS). There are many faces to this one disorder. Paradigm shifting research is linking this mind dysfunction with all of the impulsive, compulsive and addictive disorders. This means that there may be a common thread connecting as much as thirty per cent of the population. DISCOVERING RDS:
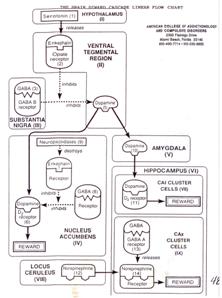
THE BRAIN REWARD CASCADE:Much like a diabetic, who has inherited a genetic predisposition to metabolic problems in their blood sugar balances, an RDS sufferer has inherited a predisposition to metabolic problems in the mind’s molecules of emotion. We all have a Brain Reward Cascade, which if operating properly is a chemical chain reaction of “neuropeptides” which excite or inhibit each other to result in feelings of wellbeing, focus, attention, reward, satisfaction, enjoyment, clarity and fulfillment. Most people are becoming used to terms such as “endorphins”, “dopamine”, and “serotonin” that are all ingredients of this chemical cascade. Put blockages in that Brain Reward Cascade and you develop a mind that lacks the ability to achieve reward and the accompanying positive functions, feelings and emotions. COMPULSIVENESS:
The problems begin when we have inherited a reward deficiency syndrome. Our inner compulsion drives us on a journey of exploration to receive the thing we need the most. When we have a lack, it puts us in a situation of experimenting with more, higher repetition, unusual, extreme, and at times illegal behaviours. And when we find the “stuff” that does it for us, or we perceive that it will give us the greatest high, then we will continue to use that stimulus, regardless of how it is perceived by others. THE LONG AND WINDING ROAD TO ADDICTION:A recovering addict has several stumbling blocks to overcome to secure a successful recovery: Withdrawal from and cravings for a substance or behaviour to which they have become dependent; repair from the damage produced by the negative consequences of their abuse; and finally a battle against something known as “abstinence-based symptoms”. David Miller, an addiction professional with 30 years experience in facilitating the recovery of numerous addicts, and himself a successful escapee from the grips of alcoholism, has found these symptoms to be the primary reason for recovery failure or relapse. And upon deeper exploration he has discovered the trend that many of these symptoms actually preceded the entry into abuse and addiction by the majority of sufferers. Abstinence-based symptoms include: restlessness, anxiety, “emptiness”, lack of energy and satisfaction (dysphoria), vague or specific cravings, depression, mental confusion, inability to concentrate and remember, irritability, sleep disturbances, and hypersensitivity to stress, sights, sounds, touch and pain (stimulus augmentation).
The Brain Reward Cascade deals with more than just emotions, having pivotal roles in attention, focus, awareness, filtration of external stimuli, responsiveness, and modulation of fight and flight mechanisms. This understanding has lead many experts to see the Limbic System as the seat of the emotions, and the home of the subconscious. You don’t usually have to think about or decide if you are going to be happy, sad, attentive, calm, or peaceful – you just are. Someone with RDS will find this achievement more difficult and will be more prone to feeling anxious, flustered, melancholy, and irritated by external sensory bombardment. One term to describe this phenomenon has been “Overload”. Built into each of us is an internal drive and desire to achieve reward – we all need to feel affection, touch, accomplishment, exhilaration, movement, exertion, and self-esteem. And we all experiment with a wide variety of behaviours and substances (natural and otherwise) to discover the ones which give us as an individual the greatest “highs”. If we imagine an RDS sufferer as someone who has a filter inside their body/mind that reduces the normal reward responses, then we start to understand that they may need to experiment with more, stronger or different inputs to attain the same level of “feel-good”. Many chronic addicts still harbour fond recollections of their honeymoon period with their substance/s of choice, some remember their first encounter as being the first time they felt euphoria and a sense of completeness. This is because many addictive substances have the ability to bind to the same receptors that normally receive the chemicals of brain reward. And most of these externally supplied chemicals produce heightened temporary feelings of everything being fun and OK.
EARLY DETECTION AND PREVENTION: One word separates use from abuse – “compulsive”. A user doesn’t spend much time in the day contemplating or planning use of a mood altering substance or behaviour. They can go out and use, or not. An abuser will look forward to use, will plan their week or day to ensure that they are in a situation where they can use, and may prioritise use over and above other normal activities. They will find that certain substances or behaviours give them a heightened sense of wellbeing that attracts them to repeatedly or increasingly use. And if they spontaneously happen on a situation that offers an opportunity to use then they will rarely say no. Two words separate abuse from addiction – “negative consequences”. When an abuser first experiences negative consequences from their habit, they may stop or at least modify that behaviour: When they get caught for drink driving they will stop or at least minimise their alcohol consumption when they are on driving duty, or they will make arrangements for transport or a place to stay so they can enjoy their use and avoid loss of their license. An addict will continue to drink and drive as their denial mechanisms will disconnect their own abuse from the consequences. They may blame others or their external circumstances for the fact they have been caught. And they will often even be convinced that they are perfectly competent to drive even when under the influence.
Watch the Discovery health Channel Documentary: Part 1...
Part 2...
TOP TEN TIPS FOR CONTROLLING RDS NATURALLY: Regardless of how you are manifesting RDS, whether ADHD, impulsive, compulsive or addictive behaviours, the recovery steps are basically the same: 1) Seek help: Make a conscious decision that today is time to get back in control of your life and mind. If you’re not ready then no-one can help you. 2) Jump start the brain reward cascade: Find a chiropractor that uses Torque Release Technique. This is a newer, gentler form of chiropractic adjustment that has been proven to drastically improve recovery outcomes, and helps to activate the Brain Reward Cascade which actually starts flowing in the spinal cord. 3) Wake up the brain reward centres: Find a practitioner that does Auriculotherapy (micro-current ear stimulation), or failing this Acupuncture. Both have long-standing histories in helping recovery and significant scientific evidence supporting their effectiveness. The ear reflex points represent the shortest neurological pathway to the brain. 4) Feed the chemistry: Access (with professional advice) some natural nutritional supplements which should include the Amino Acids: L-Tyrosine, D- and L-Phenylalanine, 5-Hydroxytryptophan, and L-Glutamine, and preferably some Magnesium and Chromium. Take these in doses recommended by your practitioner on an empty stomach to maximise their availability to your nervous system. (In some places you can even receive these intravenously.) These amino acids are the dietary building blocks to the brain chemicals of reward. 5) Balance the brain: Purchase some Binaural Beat Meditation CDs to assist your brain to enter Theta and even Delta Brain waves. Listen to these in stereo headphones. 6) Wash out the toxins: Drink heaps of filtered and alkalised water to help detoxification. 7) Replenish the nutrients: Take some multivitamins/minerals preferably in a “Green Superfood” form along with a probiotic to help repair the chemical and metabolic damage resulting from abuse. 8) Break down the denial: Consult a Counsellor and or twelve-step support group to facilitate emotional and psychological recovery. 9) Reconnect with our unreal world: Start to focus more on your spiritual side, worship your creator, pray, meditate, and connect with healthy people. 10) Take advantage of synchronicity and multiplication: Do all of the above simultaneously to maximise the healing comprehensively and to attack all angles of your RDS at the one time. TESTS FOR RDS: 1) You have completed the questionnaire in David Miller’s new book “Staying Clean and Sober” and show signs of having RDS. 2) You have been diagnosed with ADHD with psychosocial testing by a suitably qualified health care professional. 3) You have been diagnosed with a known addictive, impulsive or compulsive disorder. 4) You have had brain EEG or other electrical brain mapping tests showing the characteristic brain findings. 5) You have been genetically tested (mouth cell swab) for the genetic trait (20-30% of the population are positive). ADDICTION – HOW BIG A PROBLEM?
SUBSTANCE ABUSE: SNAPSHOTS OF THE SIZE OF THE PROBLEM:
And these make-up only a small part of the puzzle comprised of the addictive and compulsive disorders! THE INNOVATIVE USE OF MULTIPLE MODALITIES TO CONTROL ADDICTION NATURALLY: Imagine being able to relieve the ensnared anguish of victims of substance abuse. You would if you could wouldn’t you? Until recently addictions have been categorised and judged as a personal failing, but now evidence is re-educating health professionals and the community to view addictions in a new light, as a disease.
Chronic addicts are up against the statistical odds for completing a typical treatment program of 30 days. The US national retention average rate is 72%, which means out of 100 people in treatment, 28 will quit and those who finish the program stand an 85% chance of staying drug-free for 5 years. However Holder’s work has achieved a retention rate of up to 96% and even 100% when Chiropractic care was added to the therapeutic mix. So if you can get more people to finish the program, you come as close as possible to curing them, although Holder calls it “securing an ongoing recovery”, from their addictions.
Dr Nick Hodgson, a Chiropractor in private practice who coordinates Dr Holder’s training programs in Australia, is the first practitioner in Australia to offer the treatment models researched by Dr Holder. The program begins with a thorough interview and cutting edge non-invasive assessments, then using a unique diagnostic and chiropractic treatment called Torque Release Technique, which Holder is the co-developer of; Dr Hodgson determines which of the spine’s vertebrae are causing spinal cord disturbance, as every addicted person will have a subluxated spine with at least one or more vertebrae malfunctioning. Using Dr Holder’s adjustment invention, the Integrator, requiring a minimum of force and pressure, he makes a few adjustments.
“We now have a bold new approach to treating addictions that has a very high success rate and is highly cost-effective. It works so well because it removes the interference, the subluxation, to the brain reward cascade and allows you to feel good about yourself,” Dr Hodgson says. Counseling, twelve step groups and a spiritual focus are also fundamental elements of any treatment program. Chiropractic care, used in conjunction with the other modalities is offering the community and health professionals a drug-free addiction recovery program and a new understanding of addictions as a disease. It is a program that can successfully treat addicted pregnant mothers; take account of a person’s body and soul; give hope to those in the grip of addictions, be they in the workplace or in jail; claim an exceptional retention rate, and give help to communities that must pay for and deal with the consequences of addictions. A REAL-LIFE STORY:
Jack’s niece Kath hates him: why does she have to have her junky uncle living in her home? Why can’t he just get his life on track? Why can’t the many rehab centres that he has checked into keep him clean? The last thing she needs is another dysfunctional male in her life - she is trying to break things off with her "loser" boyfriend and is fighting her own struggle with depression and anorexia. Jack’s cousin Neil, on the other hand, thinks it’s kind of cool having Jack around. He likes having someone around to share a smoke or the occasional joint with - when Sue’s at work that is. Neil doesn’t see any similarity between Jack’s addiction and his own personal, “social” use of dope. But he has been finding it increasingly difficult to sleep at night, and has needed to have a few bongs by himself lately to relax. And the really bad trip he had a few nights ago at a party had made him scared: what was that stuff that his mates had given him? In the future he’d stick to the “safe” stuff. Anyway, he’d had one too many punch-ups at parties lately, and wouldn’t miss that scene for a while. The world around Jack doesn’t seem to fit. He attends many job interviews for a better class of job but there seems to be an invisible field of discrimination against him. How many times has he been told that he’s not the sort of employee they are looking for? So he ends up taking any kind of work that will accept him. Usually the sort where he doesn’t get paid enough to repay all the debts he has accumulated: his car is soon to be repossessed unless he can catch up on the six months of installments that he now owes. And all the phone and power bills that sit in a messy pile on his desk at Sue’s place just don’t seem to make sense. Things would be better if his last landlord hadn’t insisted on confiscating his bond money. How can he owe so much, to so many people? And, to make things worse, his new bosses always seem to take him for a ride in the end.
Jack knew this guy, Dr Nick, from years before, and had seen him when his back got really sore. He’d always felt better after some back manipulation so figured he had nothing to lose - after all, his back had been killing him, he couldn’t stand straight sometimes, and the headaches had become increasingly severe and common. But Dr Nick was insistent that the treatment program that he would offer Jack wasn’t just about his sore back. He believed Jack needed to commit to persisting with the treatment for weeks instead of the usual days, and that he was going to provide a mixture of therapies that nourished and repaired the mind chemical deficiencies due to Jack’s RDS. Each time Jack visited Dr Nick he received a new type of chiropractic adjustment, called "Torque Release Technique". Instead of having his neck and low-back twisted and “cracked”, it was like Justin was shooting little bolts of energy into his spine with a hand-held device. It wasn’t uncomfortable, Jack always felt really relaxed and almost sleepy after his adjustments, but he was skeptical at first because he didn’t feel like his back was getting the instant pain relief that he had experienced previously. But over the next few weeks the pain in his back and the headaches gradually subsided, and Jack felt like the fog in his mind was mysteriously clearing. Nick’s assistant would then give Jack a type of ear treatment, where she ran a high pitched device over his ear lobes, leaving him with a buzzing and at times sharp sensation. This treatment was called Auriculotherapy and had apparently evolved out of ear acupuncture, after European research had proven that it was nerve pathways that were being stimulated instead of meridian channels. This probably explained why they were using an electrical treatment instead of needles: the assistant said that it was micro-current technology, supposedly best for balancing nerve and brain function. Jack didn’t really care: he really liked the Auriculotherapy because it made him feel so relaxed, like he’d just had a nap. And for some strange reason, Jack’s cravings and withdrawals seemed so minimal compared to the other times he had attempted to go cold-turkey.
Dr Nick was seemingly always on Jack’s case about keeping his mind healthy as well: he’d recommended some meditation CDs that had special binaural tones to balance the brain waves. He was always checking on Jack to make sure he was keeping his appointments with the counselor and financial adviser, tried to convince Jack to find a 12-step support group, and even suggested that Jack should find a church group to help support him. Others noticed the changes in Jack. Sue liked to see the return of colour to her brother’s skin, and the dark rings under his eyes were fading. Kath was finding Jack easier to get along with and felt like she had gained an uncle and lost an enemy. Neil missed the free bongs that he used to score from Jack, but he too had started seeing Dr Nick to help him get back in control of his own growing dependency. And Dr Nick had made a whole lot of measurements of Jack’s spinal and nerve function, and his stress and emotional states, and these too had all visibly improved. Jack couldn’t believe how much more comfortable and steady his recovery was going this time. It just seemed like he had the strength and clarity to be able to make better choices, even when he was in tempting circumstances. It was like he just didn’t need a synthetic means of getting high and feeling good anymore. Perhaps his brain reward cascade was finally flowing again. This article is based on a true case. Names have been changed for confidentiality. ESTABLISHED METHODS WHICH HELP:
Counseling, lifestyle coaching, self-esteem building, and psychosocial methods of relapse prevention all play important roles in resolving the multi-leveled issues during recovery. The classical medical approach has been to support the psychosocial rehabilitation with a range of pharmacologic interventions to assist with pain and withdrawal management on the one hand, to replacing the substance of abuse with chemicals perceived to be more clinically and/or socially acceptable on the other. REVOLUTIONARY NATURAL TREATMENTS: Because of the complex interplay between addictive and compulsive disorders and the dependence on mood altering substances, it has been argued that the use of “therapeutic” psychoactive drugs may be counterproductive in the long term: Much like fighting fire with fire. And if the basis to these disorders is as much biological as behavioural, then solely psychosocial strategies can be frustratingly difficult for the clients: As such retention rates suffer, and the withdrawing addict is placed in an overwhelmingly difficult battle to conquer their shortcomings and to develop their willpower. What then if there were strategies to naturally bolster and repair the physiological struggles trapped inside the addict’s body, soul and spirit? There is growing evidence that this approach may actually offer the missing piece of the addiction recovery jigsaw puzzle. CHIROPRACTIC:
Recent research conducted in the United States demonstrated dramatically improved drug rehabilitation outcomes when chiropractic care was included as part of standard addiction rehabilitation. Reduced anxiety and depression levels, less need for strong pain relief and psychiatric drugs has also been a result of this treatment. Numerous research studies have shown benefits to a long list of health disorders with chiropractic care that have also highlighted recent discoveries about the chemistry and function of the central nervous system, successfully closing the gap between chiropractic theory and practice. Research suggests the spine may be an anatomical extension of the limbic system, the site where feelings are mediated. We know that many naturally occurring brain and spinal cord substances play a role in both emotions and pain reduction, leading to an increased sense of wellbeing. The role of the chiropractic spinal adjustment in removing neurological interference and in augmenting this neurological state of wellbeing is the subject of numerous past and current research projects.
Subluxation-based chiropractic treats specific sites of spinal malfunction that lead to irritation of the body’s central nervous system. There are five possible causes of a subluxation and there are five possible causes of interference to the brain reward cascade. They are the same causes, and they conduct themselves as if they were in a marriage. Therefore, if subluxations are present, a state of well-being cannot exist. By correcting subluxations we’re allowing those things that treat addiction to be embraced more thoroughly. A subluxation-free spine becomes mandatory for the expression of one’s greatest potential. AURICULOTHERAPY: Auriculotherapy is a therapeutic intervention in which stimulation of the auricle of the external ear is used to alleviate health conditions in other parts of the body. While originally based on the ancient Chinese practice of acupuncture, the somatotopic correspondence of specific parts of the body to specific parts of the ear was first developed in France. In 1957 Dr Paul Nogier, a physician from Lyon observed the occurrence of scars on the ear of patients who had been treated successfully for sciatica pain by lay practitioners. Dr Nogier’s subsequent research led to the ‘somatotopic’ map of the ear, based on the concept of an inverted fetus (upside-down baby) orientation. Research studies in China and the US verified the scientific accuracy of auricular diagnosis. In China the ear points of over 2,000 patients were assessed, recording which points correlated with certain diseases and ear points lead to reduction of medical symptoms.
Microcurrent is used in preference to needles, acupressure, laser and other forms of current (e.g. TENS), as this best matches the natural frequencies of the nerves being treated. Hence Micro-current is attempting to normalize abnormal nerve activities. The design features of modern Auriculotherapy instruments (e.g. StimplusPro) have the advantage of being able to locate the active reflex points, as well as treat. Auriculotherapy offers advantages over the more traditionally utilised ear acupuncture in reduced costs with no disposable needles, less practitioner contact time, reduced infectious disease risks as there is no skin piercing, improved diagnosis and location of points, removal of the psychosocial issue of using needles in this population, reduced treatment time, utilisation of internationally and scientifically accepted treatment points. Research suggests that this modality assists with issues of withdrawal, craving, pain management, depression, anxiety, and impulsiveness. Long term follow up of drug related offenders showed amazing reduction in the number of re-arrests in those who received Auriculotherapy as part of their rehabilitation and hence should be made available on a regular ongoing basis during the recovery process. NEUTRICEUTICALS: Neutriceuticals are nutrients used at levels to achieve pharmacologic like changes in the body in order to aid the brain and nervous system to increase the level of chemicals necessary to make specific neurotransmitters. These same neurotransmitters are also deficient in ADHD sufferers. These messengers communicate a feeling of calmness and wellbeing to the brain.
Combinations of select high quality amino-acids, glycoproteins, vitamins and minerals have been shown to measurably increase certain important neurotransmitters in the brain. These include serotonin, endorphins, dopamine, GABA; the four neurotransmitters responsible for brain reward. Dopamine, when it works in the part of the brain called the ‘reward site’, is considered the pleasure molecule and the anti-stress molecule. Aberrant craving behaviour for all forms of cocaine and amphetamines occur when there is a deficiency of brain dopamine. The amino-acid and related formulas can be designed to bring about natural feelings of well-being; provide nutritional support in recovery for those with RDS; reduce post-abstinence withdrawal symptoms including cocaine dreams; reduce cravings; reduce stress responses. OTHER NATURAL MODALITIES: Any number of natural therapies ranging from full-body acupuncture to massage, vitamin supplements to structured dietary regimes, exercise to meditation, hypnosis to prayer can also be argued to be of benefit to the recovering addict. Each should be carefully considered in the management of each individual case, and preference should be given to modalities with some evidence of clinical benefit. PIECING TOGETHER THE RECOVERY JIGSAW PUZZLE:
For example the Chiropractor just offering subluxation correction to an addicted patient would be leaving that person in a vulnerable position, attempting to handle their withdrawal, social, spiritual and psychological recovery alone. A psychologist or counselor believing they can rehabilitate the behavioural inconsistencies and flawed self-belief systems will be guaranteeing the client an uncomfortable and incomplete recovery of their brain reward systems, without the strategies to fill this biological void. The medical professional offering pharmacologic intervention only, may be contributing to the substitution of one substance abuse for another. And the case managers, social workers, and carers helping the addict to piece their life back together; may remain trapped in the frustrating world of repeated withdrawal and relapse unless supported by a team of professionals positioned to improve clinical outcomes. RECOVERY RECOMMENDATIONS: A recovery program should provide a multimodal, holistic process which maximises recovery from the negative consequences of substance abuse, maximises opportunity for sustained abstinence, minimises risk of relapse, and restores a healthy state of wellbeing. The multimodal approach combines accepted psychosocial methods of assisting recovery, with some less “mainstream” evidence-based complementary health care practices. RECOVERY SERVICES OVERVIEW:
PROGRAM OVERVIEW: The services provided will be prescribed in a manner deemed clinically necessary to maximise the chances of sustained abstinence and continued recovery. In general clients should initially be attending group 1-2 times weekly, attending counseling at least once weekly, receiving Auriculotherapy and Chiropractic care three times weekly, taking supplements daily, exercising 3-4 times weekly - The regularity and timing of each activity will be reviewed and modified each 30 days. OUTCOME ASSESSMENTS: A mixture of outcome tools will be utilised to assess success of recovery in the following areas: 1) Retention rates: 2) Signs of relapse: Symptoms of depression and anxiety have been implicated in probabilities of relapse. These symptoms will be observed with the expectancy of progressive reduction throughout the program: Depression and Anxiety questionnaires will be administered at least monthly to quantify symptoms. 3) State of wellbeing: Patients who display a high “state of wellbeing” would be considered to be at decreased risk of relapse and failure. Measures of this state would be expected to increase throughout the program: Blanks state of wellbeing inventory will be administered at least monthly to quantify the patient’s state of wellbeing. 4) Physiological markers: Non-invasive tests may be administered which are utilised as outcome assessments for the clinical effectiveness of the complementary (“CAM”) health care services: These markers individually and collectively would be expected to progressively improve throughout the program if the CAM modalities are assisting the recovery process. a) Postural assessment. b) Spinal flexibility measurement. c) Paraspinal surface electromyography. d) Paraspinal infrared thermography e) Brain EEG f) Heart Rate Variability
SPECIAL NEEDS:
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Main Page About TRT The Integrator Research Directory TRT Training Testimonials BLOG Products Site Map Contact Us Torque Release Technique (TRT) is the first Chiropractic Technique to be created through a rigorous scientific research and development process. TRT aims to improve health and wellbeing by improving Nervous System function via specific Adjustment of Primary Subluxations. TRT is an extremely gentle chiropractic method and has been published in major Medical and Chiropractic Journals and featured on the Discovery Health Channel. © Dr Nick Hodgson 2008 2005 Victorian Chiropractor of The Year, Australasian TRT Training Provider, Fellow Holder Research Institute. Visit Nick's other web site at www.superhealthy.com.au |
|






 The
primary human compulsion is the need for reward: Brain reward is
our highest payment – more valuable than gold and dollars. The sum total of each
individual’s habits and repetitive behaviours is the result of the perceived
rewards that we receive or desire from the planet, the people around us and our
own thoughts, actions and intakes.
The
primary human compulsion is the need for reward: Brain reward is
our highest payment – more valuable than gold and dollars. The sum total of each
individual’s habits and repetitive behaviours is the result of the perceived
rewards that we receive or desire from the planet, the people around us and our
own thoughts, actions and intakes. Just
as a person with the genetic trait for diabetes doesn’t wake one morning a
diabetic; an RDS sufferer doesn’t suddenly become an addict. The symptoms of
abstinence and the symptoms of RDS are one and the same, and bear common themes
with the symptoms of ADHD. The behaviours associated with ADHD are well-publicised
and caricatured, and produce an all-too prevalent diagnostic trend. But to
understand how someone with RDS and/or ADHD is predisposed to become an addict
we need to understand what it feels like on the inside to live with this human
variant.
Just
as a person with the genetic trait for diabetes doesn’t wake one morning a
diabetic; an RDS sufferer doesn’t suddenly become an addict. The symptoms of
abstinence and the symptoms of RDS are one and the same, and bear common themes
with the symptoms of ADHD. The behaviours associated with ADHD are well-publicised
and caricatured, and produce an all-too prevalent diagnostic trend. But to
understand how someone with RDS and/or ADHD is predisposed to become an addict
we need to understand what it feels like on the inside to live with this human
variant. And
in the early days this feels like a good thing, often the best thing ever to
that person. Some even find that while they are under the influence of their
new-found best friend, they function, relate to, and perform better within the
home, the workplace and society. But this love affair is not one of
interdependency and growth. The all too common trend is that the user becomes an
abuser, as they find that larger quantities and more regular intake is required
to continue to achieve the same degree of fulfillment. The body is not stupid.
As we synthetically supplement our deficient reward process, our body adapts to
the strong stimuli and moves towards tolerance. Some of the synthetic chemicals
are poorly digested and continue to bind and block the receptor sites. At the
same time the body reduces the production of its own “endogenous” reward
chemicals, initiating the downward spiral towards addiction. Why should it make
its own chemicals when we are inhaling, ingesting, injecting or obsessively
bombarding them instead?
And
in the early days this feels like a good thing, often the best thing ever to
that person. Some even find that while they are under the influence of their
new-found best friend, they function, relate to, and perform better within the
home, the workplace and society. But this love affair is not one of
interdependency and growth. The all too common trend is that the user becomes an
abuser, as they find that larger quantities and more regular intake is required
to continue to achieve the same degree of fulfillment. The body is not stupid.
As we synthetically supplement our deficient reward process, our body adapts to
the strong stimuli and moves towards tolerance. Some of the synthetic chemicals
are poorly digested and continue to bind and block the receptor sites. At the
same time the body reduces the production of its own “endogenous” reward
chemicals, initiating the downward spiral towards addiction. Why should it make
its own chemicals when we are inhaling, ingesting, injecting or obsessively
bombarding them instead? From
here things can only get worse: Now we need to take our “stuff” just to feel OK,
and if we continue the abuse or even start to layer on more forms of abuse in a
vain attempt to find new rewards we regress to the point of not even feeling
good when we are using: But somewhere imprinted in our subconscious is the
memory and the uncontrollable desire that it just might work again. This is why
recovery can never be solely a process of conscious decision, willpower or
better choices. One sufferer described it as though she had two brains: One that
recognised the negative consequences and costs of the abusive behaviours and
substances that she had become embroiled in, then this other “mind” that wanted
to feel the way she did when she first started using. She would set out with the
best intentions driven by her conscious mind, but would eventually be persuaded
by this internal voice that convinced even her purest intentions that it would
be OK and necessary for survival to use one more time.
From
here things can only get worse: Now we need to take our “stuff” just to feel OK,
and if we continue the abuse or even start to layer on more forms of abuse in a
vain attempt to find new rewards we regress to the point of not even feeling
good when we are using: But somewhere imprinted in our subconscious is the
memory and the uncontrollable desire that it just might work again. This is why
recovery can never be solely a process of conscious decision, willpower or
better choices. One sufferer described it as though she had two brains: One that
recognised the negative consequences and costs of the abusive behaviours and
substances that she had become embroiled in, then this other “mind” that wanted
to feel the way she did when she first started using. She would set out with the
best intentions driven by her conscious mind, but would eventually be persuaded
by this internal voice that convinced even her purest intentions that it would
be OK and necessary for survival to use one more time.


 Dr
Jay Holder of the Holder Research Institute in Miami has led the way for close
to 30 years with his research and educational programs at the American College
of Addictionology and Compulsive Disorders, training and certifying
professionals to work as Addictionologists. Holder,
who is a Certified Addictionologist and Chiropractor directing two chiropractic
clinics and two addiction recovery facilities, has invented medical devices,
formulas, published research and run educational programs in the US, Israel, the
UK and Australia expounding his innovative approaches.
Dr
Jay Holder of the Holder Research Institute in Miami has led the way for close
to 30 years with his research and educational programs at the American College
of Addictionology and Compulsive Disorders, training and certifying
professionals to work as Addictionologists. Holder,
who is a Certified Addictionologist and Chiropractor directing two chiropractic
clinics and two addiction recovery facilities, has invented medical devices,
formulas, published research and run educational programs in the US, Israel, the
UK and Australia expounding his innovative approaches. Next,
Dr Hodgson uses a range of amino acids, precursors to or building blocks for
proteins, normally found in foods and taken daily as oral supplements. These can
include 5-Hydoxytryptophan, L-Phenylalanine, D-Phenylalanine, l-Glutamine and
L-Tyrosine. The amino acids are necessary precursors for the brain reward
cascade chemicals, or neurotransmitters, known through the work of Holder’s
colleague, Kenneth Blum, PhD of the University of Texas Health Science Centre,
that are chronically deficient in the addicted person. Blum determined that
specific combinations of amino acids could help to balance and restore the
linear sequence of brain chemicals in the brain reward cascade function.
Next,
Dr Hodgson uses a range of amino acids, precursors to or building blocks for
proteins, normally found in foods and taken daily as oral supplements. These can
include 5-Hydoxytryptophan, L-Phenylalanine, D-Phenylalanine, l-Glutamine and
L-Tyrosine. The amino acids are necessary precursors for the brain reward
cascade chemicals, or neurotransmitters, known through the work of Holder’s
colleague, Kenneth Blum, PhD of the University of Texas Health Science Centre,
that are chronically deficient in the addicted person. Blum determined that
specific combinations of amino acids could help to balance and restore the
linear sequence of brain chemicals in the brain reward cascade function. Using
new information about the energetics of the ear, Auriculotherapy, Dr Holder has
further refined the five ear points described in Classical Chinese medicine
identifying three completely new points for all addiction treatments. These are
related to the four cranial nerves that have nerve endings throughout the ear.
However, again Holder uses an innovative technique that does not require needles
called a StimPlus Pro 103F, which is a small handheld probe that delivers
specific frequencies in micro-current to specific ear points for 30-60 seconds
per point. This is a highly efficient and specific therapy, and helps release
the pleasure-producing brain chemicals, endorphins, more quickly and more
thoroughly than needle treatment when clients need an energy boost to lift
depression, cut drug cravings, increase relaxation and improve compliance.
Using
new information about the energetics of the ear, Auriculotherapy, Dr Holder has
further refined the five ear points described in Classical Chinese medicine
identifying three completely new points for all addiction treatments. These are
related to the four cranial nerves that have nerve endings throughout the ear.
However, again Holder uses an innovative technique that does not require needles
called a StimPlus Pro 103F, which is a small handheld probe that delivers
specific frequencies in micro-current to specific ear points for 30-60 seconds
per point. This is a highly efficient and specific therapy, and helps release
the pleasure-producing brain chemicals, endorphins, more quickly and more
thoroughly than needle treatment when clients need an energy boost to lift
depression, cut drug cravings, increase relaxation and improve compliance. According
to Blum and Holder there are two key factors causing addictions the first of
which is a genetic flaw called “the A1 allele of the D2 dopamine receptor” found
in 69% of severe alcoholics. The second cause, according to Holder’s research,
is that an estimated 90% of babies born through a difficult or assisted delivery
arrive with a spinal subluxation, and if the infant has the genetic defect as
well, then the chances of becoming an addicted adult are very high. The
connection between a subluxated spine and addictions is linked to the sequence
of chemical changes in your brain, which if released in the right sequence make
you feel good, but if the sequence is interfered with, may prompt the search for
mood-altering substances to make you feel good.
According
to Blum and Holder there are two key factors causing addictions the first of
which is a genetic flaw called “the A1 allele of the D2 dopamine receptor” found
in 69% of severe alcoholics. The second cause, according to Holder’s research,
is that an estimated 90% of babies born through a difficult or assisted delivery
arrive with a spinal subluxation, and if the infant has the genetic defect as
well, then the chances of becoming an addicted adult are very high. The
connection between a subluxated spine and addictions is linked to the sequence
of chemical changes in your brain, which if released in the right sequence make
you feel good, but if the sequence is interfered with, may prompt the search for
mood-altering substances to make you feel good. Jack
is depressed, and is becoming increasingly frustrated. And things aren’t
improving. Each time he tries to overcome his addiction to marijuana and then
relapses, the feelings of failure, desperation, disconnection and hopelessness
increase. But Jack’s struggle isn’t just destroying his own life. His sister Sue
is tired: tired of Jack disappearing in search of fulfillment of his compulsive
need for “relief”; tired of him reappearing in a dark, disheveled, unwell and
dirty state; tired of dealing with the calls from authorities telling her to
come and get him; tired of the angry outbursts, the coughing and hacking through
the night as Jack dries out once again.
Jack
is depressed, and is becoming increasingly frustrated. And things aren’t
improving. Each time he tries to overcome his addiction to marijuana and then
relapses, the feelings of failure, desperation, disconnection and hopelessness
increase. But Jack’s struggle isn’t just destroying his own life. His sister Sue
is tired: tired of Jack disappearing in search of fulfillment of his compulsive
need for “relief”; tired of him reappearing in a dark, disheveled, unwell and
dirty state; tired of dealing with the calls from authorities telling her to
come and get him; tired of the angry outbursts, the coughing and hacking through
the night as Jack dries out once again.  Jack
was lucky; he had been helped by some good people. His older brother Rod had
been a solid influence and had helped to "clean up" Jack on a number of
occasions. He lived too far away to be there all the time but his background in
success thinking, and his influence on Jack to clean up his diet, take some
vitamins, and drink much more water had helped to improve Jack’s general health
- but the addiction remained. The counselors meant well and Jack didn’t mind
talking about the struggles he had as a teenager - he felt like he had never
totally fitted in to the “normal mould” and it was therapeutic to get some of
this stuff off his chest. And the financial adviser was helping him to get his
debts repaid a little at a time. But then his sister had insisted that he go and
have a chat with a natural health practitioner who had been receiving training
from overseas in radical and alternative treatment strategies for people just
like himself.
Jack
was lucky; he had been helped by some good people. His older brother Rod had
been a solid influence and had helped to "clean up" Jack on a number of
occasions. He lived too far away to be there all the time but his background in
success thinking, and his influence on Jack to clean up his diet, take some
vitamins, and drink much more water had helped to improve Jack’s general health
- but the addiction remained. The counselors meant well and Jack didn’t mind
talking about the struggles he had as a teenager - he felt like he had never
totally fitted in to the “normal mould” and it was therapeutic to get some of
this stuff off his chest. And the financial adviser was helping him to get his
debts repaid a little at a time. But then his sister had insisted that he go and
have a chat with a natural health practitioner who had been receiving training
from overseas in radical and alternative treatment strategies for people just
like himself. Then
Jack felt he made real breakthrough. Dr Nick had given him a bottle of
vitamin-type capsules that Jack had to take three times a day on an empty
stomach. These capsules contained amino acids, minerals and a few vitamins -
stuff that Nick said were the building blocks of the mind chemicals that were
deficient in the majority of RDS sufferers. Jack couldn’t be sure that it was
the capsules, or whether it was the combination of things that he was trying,
but seemingly days after starting the “nerve food” as Nick called it, his mind
just seemed clearer and more focused. He even sat at his desk and organised the
pile of bills into the order in which they most needed to be paid.
Then
Jack felt he made real breakthrough. Dr Nick had given him a bottle of
vitamin-type capsules that Jack had to take three times a day on an empty
stomach. These capsules contained amino acids, minerals and a few vitamins -
stuff that Nick said were the building blocks of the mind chemicals that were
deficient in the majority of RDS sufferers. Jack couldn’t be sure that it was
the capsules, or whether it was the combination of things that he was trying,
but seemingly days after starting the “nerve food” as Nick called it, his mind
just seemed clearer and more focused. He even sat at his desk and organised the
pile of bills into the order in which they most needed to be paid. We
know that addiction to drugs involves three important basic elements: The
physiological, psychological, and spiritual. Any treatment and/or recovery
begins with the acceptance that one cannot control the disease and assistance is
required, thus invoking a well established pattern that leads to the Twelve
Steps program or other similar spiritual guidelines.
We
know that addiction to drugs involves three important basic elements: The
physiological, psychological, and spiritual. Any treatment and/or recovery
begins with the acceptance that one cannot control the disease and assistance is
required, thus invoking a well established pattern that leads to the Twelve
Steps program or other similar spiritual guidelines. Chiropractic
emphasizes the inherent recuperative power of the body to heal itself without
the use of drugs or surgery. The practice of chiropractic focuses on the
relationship between structure (primarily of the spine) and function (as
coordinated by the nervous system) and how that relationship affects the
preservation and restoration of health. The foundation of chiropractic has
always rested on the supremacy of the neurological systems over every other body
system, and that Chiropractic intervention aims to improve neurological
function.
Chiropractic
emphasizes the inherent recuperative power of the body to heal itself without
the use of drugs or surgery. The practice of chiropractic focuses on the
relationship between structure (primarily of the spine) and function (as
coordinated by the nervous system) and how that relationship affects the
preservation and restoration of health. The foundation of chiropractic has
always rested on the supremacy of the neurological systems over every other body
system, and that Chiropractic intervention aims to improve neurological
function.
 Auriculotherapy
is sometimes referred to as ear acupuncture but it uses no needles and does not
rely on the meridian system. A microcurrent stimulator is placed on reflex
points on the outside of the ear. These points then send a message to the brain
based on the location of the reflex point being treated. Most people feel only a
tiny tingling at the ear reflex points during treatment.
Auriculotherapy
is sometimes referred to as ear acupuncture but it uses no needles and does not
rely on the meridian system. A microcurrent stimulator is placed on reflex
points on the outside of the ear. These points then send a message to the brain
based on the location of the reflex point being treated. Most people feel only a
tiny tingling at the ear reflex points during treatment. Addiction-free
behaviour is facilitated by the availability of enzymes to regulate the supply
of brain chemicals such as an adequate supply of neurotransmitters, and the
presence of receptors to give neurotransmitters access to the neurons that
determine feelings of wellbeing. A malfunction in any of these areas may trigger
a compulsive biogenic disorder.
Addiction-free
behaviour is facilitated by the availability of enzymes to regulate the supply
of brain chemicals such as an adequate supply of neurotransmitters, and the
presence of receptors to give neurotransmitters access to the neurons that
determine feelings of wellbeing. A malfunction in any of these areas may trigger
a compulsive biogenic disorder. Once
one grasps the genetic and neurobiological contribution to addictive and
compulsive behaviours, and adds to this the vast psychosocial aspects involved
in the development of crippling, long term illness; it becomes apparent that
specialised and advanced recovery strategies are required from a wide range of
craft-groups to symbiotically contribute to effective solutions for the addicted
client.
Once
one grasps the genetic and neurobiological contribution to addictive and
compulsive behaviours, and adds to this the vast psychosocial aspects involved
in the development of crippling, long term illness; it becomes apparent that
specialised and advanced recovery strategies are required from a wide range of
craft-groups to symbiotically contribute to effective solutions for the addicted
client.





